

Abstract
Background: Immune reconstitution after allogeneic stem cell transplantation (SCT) is a complicated process influenced by factors such as preconditioning regimens, graft-versus-host disease (GVHD) prophylaxis, and grafts. We studied the association between the kinetics of lymphocyte subsets and transplant outcome to clarify the differences in immune reconstitution after hematopoietic cell transplantation according to stem cell sources and its clinical significance.
Patients and Methods: Clinical data were collected from patients' medical charts at Kanagawa Cancer Center, Yokohama, Japan. Patients with hematological malignancies aged ≥18 years old who underwent SCT between April 2009 and December 2017 were initially selected. Those who died or experienced disease relapse before day 100 post SCT were excluded. We measured absolute lymphocyte count (ALC) and lymphocyte subsets by flow cytometry with antibodies against CD2, CD3, CD4, CD8, CD11b, CD11c, CD16, CD25, CD29, CD56, CD57, CD45RA, and CD45RO on days 100, 180, 365, and 730 post SCT.
Results: The final cohort included 314 patients (acute leukemia, n = 249; myelodysplastic syndrome, n = 44; chronic myelogenous leukemia, n = 9; malignant lymphoma, n = 6; and others, n = 6). The median age was 51 (range: 18- 69) years, with 184 males and 130 females. The disease risk at transplantation was standard in 209 and high in 105 patients. Myeloablative preconditioning was administered to 114 and reduced-intensity preconditioning to 200 patients. Bone marrow transplantation (BMT), peripheral blood SCT (PBSCT), and cord blood transplantation (CBT) were performed in 121, 57, and 136 patients, respectively. A calcineurin inhibitor with short-term methotrexate was mainly used for GVHD prevention. The median follow-up of surviving patients was 869 (range: 103-3074) days. The 2-year overall survival (OS), cumulative incidence of relapse (CIR), and non-relapse mortality (NRM) in BMT, PBSCT, and CBT were 62%, 68%, and 76% (P = 0.023); 33%, 38%, and 27% (P = 0.068); and 17%, 16%, and 13% (P = 0.82); respectively. The 2-year cumulative incidence of chronic GVHD was 43% in BMT, 45% in PBSCT, and 28% in CBT (P = 0.027).
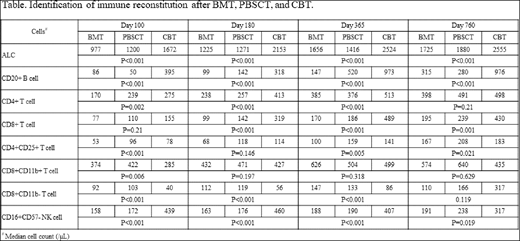
There were significant differences between lymphocyte subset recovery and stem cell sources (Table). ALC; CD20+ B cell; CD4+, CD4+CD29+, CD4+CD45RO+, CD4+CD45RO− , and CD4+CD45RA+ T cell subsets; and CD3−CD56+ and CD16+CD57− natural killer (NK) cell subsets were significantly elevated in CBT compared with BMT and PBSCT at day 100 post SCT. Conversely, CD8+CD11b+ and CD8+CD11b− T cell subsets and CD3+CD56+ NKT cells were significantly lower in CBT than in BMT and PBSCT on day 100. Univariate analysis revealed that lymphocyte subsets exhibiting higher levels of CD20+ B cell; CD16+CD57− and CD3−CD56+ NK cells; and CD4+CD25+, CD4+CD29+, CD4+CD45RA+, CD8+CD11b+, and CD8+CD11b− T cell subsets at day 100 were associated with a better 2-year OS. There were strong correlations with a lower CIR and higher CD16+CD57+ and CD16+CD57− NK cell levels . A higher incidence of chronic GVHD was associated with lower levels of CD16+CD57− NK cells and CD4+CD25+ T cells and with higher levels of CD8+CD11b+ T cells and CD8+CD11b− and CD3+CD56+ NKT cells. Further, a lower NRM correlated with higher levels of CD20+ B cells and CD8+CD11b− T cells.
The lymphocyte subsets were used for multivariate analysis. Favorable factors for better OS were higher levels of CD16+CD57− NK cells [hazard ratio (HR), 0.62; 95% confidence index (CI), 0.38-0.81; P = 0.024] and CD20+ B cells (HR, 0.56; 95% CI, 0.31-0.0.98; P = 0.048). Prognostic factors for lower CIR were higher levels of CD16+CD57+ NK cells (HR, 0.51; 95% CI, 0.27-0.95; P = 0.034) and CD16+CD57− NK cells (HR, 0.52; 95% CI, 0.28-0.99; P = 0.048). A lower incidence of NRM was associated with higher levels of CD8+CD11b− T cells (HR, 0.18; 95% CI, 0.08-0.39; P < 0.001) and CD20+ B cells (HR, 0.24; 95% CI, 0.08-0.70; P = 0.0088). High levels of CD8+CD11b+ T cells were an independent predictor for a higher incidence of chronic GVHD (HR, 2.38; 95% CI, 1.22-4.95; P = 0.012).
Conclusions: The distinct differences in immune reconstitution according to stem cell sources and lymphocyte subset analysis at day 100 post SCT are useful for predicting transplant outcome. Furthermore, the results suggest that characteristic immune recovery in CBT positively affects transplant outcome.
No relevant conflicts of interest to declare.

